Written by Dr Guy Hatchard
A look at the New Zealand data released under OIA
Hundreds of deaths associated with vaccination
Lessons can be learned. National reconciliation is possible
This release presents the association between weekly vaccination totals and all-cause mortality for the 60+ age cohort. We can make this association because of our unique situation in NZ. Protected at our borders, we have a very low incidence of Covid, and therefore, the short-term impact of vaccination on health can be reviewed in isolation from the confounding factors of Covid infections and deaths.
Writing this has been a painful release because it involves personal tragedies affecting families and loved ones. Some of them are not aware of the causes of their loss or, in other cases, have been misled through preventable mistakes of government and civil servants. It has been clear for some time that the rate of adverse effects proximate to mRNA Covid vaccination is unprecedented throughout NZ vaccination history. Adverse effects reported to CARM are running at 30 times that of flu vaccines. It is also apparent that many of the adverse effects are very serious.
Medsafe has continued to maintain that they cannot determine which effects and deaths are related to vaccination. However, I have previously written about indications pointing to a causal relationship between various adverse effects and vaccination. These effects range from those already admitted, such as myocarditis, to those recognised in a leaked Pfizer document dated April 30th 2021, including respiratory illness, internal bleeding, kidney and liver disease, neurological disease, thrombotic events, stroke, and immune suppression, and many more. This list is not exhaustive.
What does Dr Ashley Bloomfield have to say?
On October 28th, I wrote to Dr Ashley Bloomfield, pointing to the unusually high level of adverse effects and requesting that reporting of adverse effects should be mandatory rather than voluntary. Yesterday, December 17th, I received a tardy reply from Astrid Koorneef, Director of the National Immunisation programme, writing on behalf of Dr Ashley Bloomfield. In this, Astrid specifically rejects my request saying: “An accurate measurement of all adverse events is not required” and further suggested I confine myself to trusting MoH websites rather than public domain sources. Her letter offered this view of the determination of causal relationships:
“We are aware of reports circulating in social media where an adverse event has a temporal association with the vaccination. This is not indicative of a causal relationship to the vaccine. Causal relationships between AEFIs and the vaccine are established through robust pharmacovigilance examinations that take into consideration global reporting of the adverse event, the background rate for the condition, and safety signal analysis.”
In other words, Ashley Bloomfield wants us to believe that an adverse effect rate 30 times that of the flu vaccine is a coincidence. Yet Hill’s standard criteria of medical causality include repeated temporal association as criteria of greatest importance. He discusses this first in his seminal text still in use today. As Astrid asserts on behalf of MoH, it cannot be reasonably held that such associations are not indicative. As a scientist, the first evidential alert to causality is always temporal association. Of necessity, the association should prompt further investigations. Scientists then ask questions such as Is the association plausible? Does it occur in different settings? Are rates of occurrence significant? Mandatory reporting is essential. Astrid refers to the need for robust pharmacovigilance; this is the name given to safety and assessment protocols used in drug trials. In drug trials, mandatory reporting is always required. Astrid also states:
“The Cominarty [Pfizer mRNA vaccine] has completed all testing requirements.”
This is not the case. The Pfizer vaccine only has an emergency or provisional approval worldwide. The purpose of a long period of pharmacovigilance (always several years) includes the need to ascertain the extent of secondary health effects of the vaccine. Without mandatory reporting, the identification of related adverse effects will remain incomplete. There is an obvious need to investigate vaccine safety here in NZ because overseas trials are as yet preliminary—the long term effects of mRNA vaccines are unknown, and the short term effects are incompletely assessed.
The data released under OIA
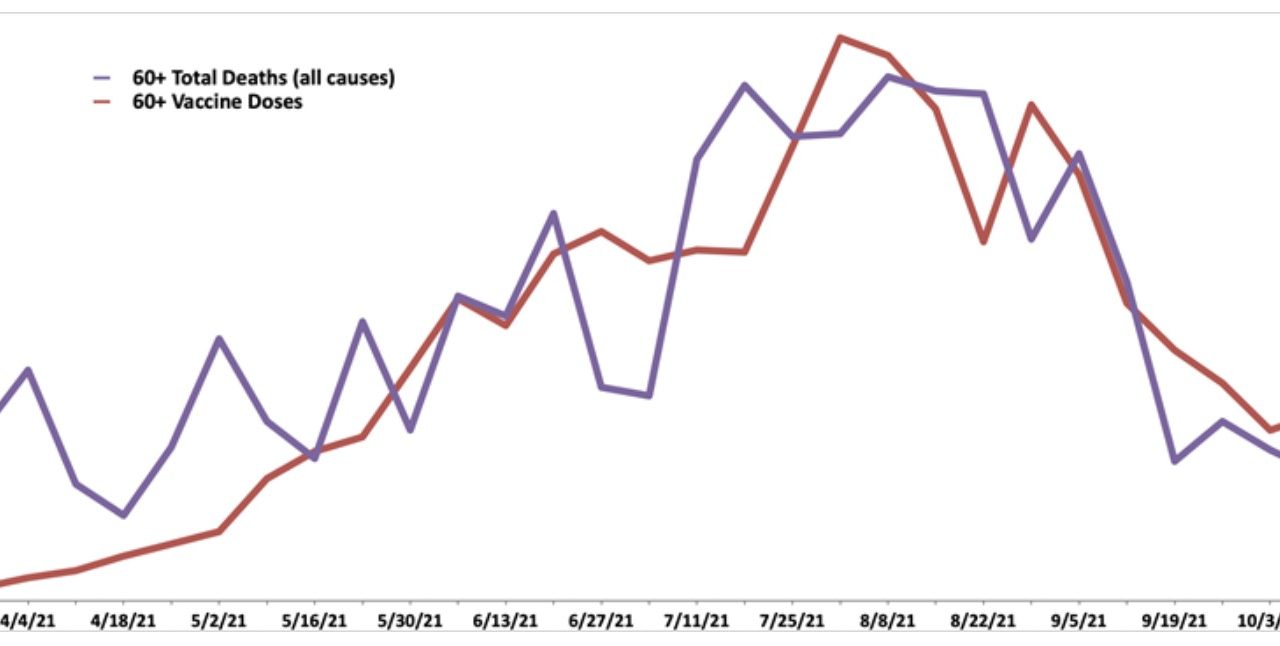
Grant Dixon obtained figures from Medsafe through an OIA request graphed here:
The temporal association between all-cause deaths and vaccination for the 60+ age cohort during the rollout of the mRNA vaccine in NZ between the beginning of March 2021 to the end of October 2021 is graphically rather obvious even to a layperson. As weekly vaccination numbers rise to a peak, deaths peak. As vaccination numbers begin to fall, deaths also fall. The number of excess deaths in the weeks following vaccination is consistent with reports of 670 suspicious deaths proximate to vaccination submitted voluntarily to NZDSOS and NZ Health Forum and could be more significant.
Further investigation requires a comparison between adverse effect rates and expected incidence of disease by category and also an examination of the potential mechanisms for disease creation in so far as they are known. Medsafe recently rejected any association because it compared death rates by disease categories to prior years 2008 to 2019 and found them similar. Our review of the historical data reveals that Medsafe’s comparison was not the appropriate choice because it went back too many years when death rates were higher and crucially ignored the lockdown conditions. 2020 deaths rates, when conditions were similar to 2021, are much lower than historical data. As to mechanisms, the actions of the mRNA vaccine and the spike protein it produces are still the subject of copious ongoing research, vigorous debate, and publication. Therefore, the graphical association is a preliminary but robust indication. We are commenting on the data because of the urgent need to inform the public and strike a note of caution that has been absent from government vaccination publicity.
The data raises important questions for the government:
Why has Medsafe failed to take the apparent association between vaccination and all-cause mortality and the very high adverse event tally seriously? This is hard to understand but par for the course. A letter sent by Dr Ashley Bloomfield and Dr Andrew Connolly to DHB organisers dated December 15th 2021, pressed the emergency button concerning the incidence of myocarditis and pericarditis and admitted underreporting.
What is important here is that the MoH has known about the risk of such cardiac illness since early in the year, but it took ten long months before they wrote to DHBs to alert them that the threat was severe enough for them to organise a concerted response.
Why did Medsafe, MoH and Dr Ashley Bloomfield promote the mistaken idea that temporal association is not an indication of causality? A false premise bolstered their public narrative that the high tally of deaths proximate to vaccination was coincidental.
Why didn’t MoH instruct GPs and hospital staff to report all adverse effects? In fact, in the absence of straightforward advice, the opposite has happened. For example, the Medsafe mRNA vaccine fact sheet mentions only 21 side effects, all except three of which are mild. This has resulted in a high percentage of vaccine injury cases going unreported and the injured themselves being told by GPs and hospital staff they are suffering from anxiety or imagination or new unrelated conditions.
Why have GPs been reluctant to report adverse effects or inform their patients of risks? The fault lies with a government policy to discourage and discipline doctors questioning vaccine safety. As a result, GPs are very understandably afraid to speak out when they see their colleagues being disciplined for striking a cautious note with their patients. Moreover, their customary role in granting exemptions was taken away from them.
In Medsafe’s case by case investigation of deaths, why didn’t they recognise that our knowledge of mRNA vaccine adverse effects and the mechanisms that cause them has been growing, especially in genomics?
Why did Medsafe, government advisors, and Jacinda Ardern ignore the enormous volume of social media reports of adverse effects and dismiss them as inconsequential and accuse those reporting of unreliability or worse? After all, Jacinda Ardern and the government can certainly dish out social media myths. So why regard public feedback as irrelevant?
Why is our government still blasting out a message of complete safety over the airwaves, especially considering the alarmed tone of the private DHB message from Dr Bloomfield? How did the government think it was ethical to mislead the population? This has confused those adversely affected by vaccination. In some cases, it has prevented individuals from realising they urgently needed medical assistance.
What are the lessons to be learned?
Because of NZ border controls, we can assess vaccine effects in isolation from Covid itself, but it was inappropriate and disappointing to receive the reproving message from MoH yesterday, which was worthy of a crime scene drama—move along, sir, there is nothing to be seen here. There was no acknowledgement of vaccine harm. Comparing the two letters sent to me and one to DHB heads on the same date, the intent is clear—try to dampen public disquiet with misleading messaging while privately giving way to something close to an emergency. Were the continuing efforts to keep the public message on vaccine safety separate from the science the result of a political decision taken by Jacinda Ardern’s government, or was it a result of MoH advice? Was this policy adhered to because of a perceived need to promote a public good?—the arguments for which have long since left science behind (something we have argued elsewhere). We are a small country. We talk to one another. How could the government think that contradictory messaging could be maintained without public knowledge? What are key lessons to be learned?
Firstly, numerous scientists were warning our government about the need for caution and constant review; these included members of the Skegg Committee, Michael Baker, and others. Certainly, they should have gone further, but even so, why did the government decide to mandate vaccination as a virtually stand-alone solution? Was it because vaccination was presented to them as the only possible solution? Did our government and Medsafe surrender too easily to commercial vaccine narratives originating overseas? Did they ignore the growing catalogue of adverse effects recorded around the world?
Secondly, why did the government double down with vaccine mandates while the research showed that vaccines were less and less effective? Why did they not cast around for other more promising or complementary public messaging? The single most important message of the pandemic has been that severe Covid illness is connected to comorbidities. Given that we had some protection at our border, which gave us time, why did my government correspondents reject a robust public health campaign and legislative programme that emphasised preventive health measures?
Thirdly, it is now clear that hesitant vaccine people had good reason to be hesitant. Why was this not acknowledged as soon as the virtual tsunami of adverse effects became apparent? It is hard to escape the notion that resolutely maintaining that the vaccine was safe in the public messaging was a coordinated conspiracy of silence. Finally, it is not clear why people experiencing an adverse reaction to the first vaccine dose were refused an exemption for the second—a policy Dr Ashley Bloomfield has personally and rigidly enforced. This is especially egregious considering the government was aware of overseas research findings that the double dose causes a stronger reaction.
Fourthly, we have resources in NZ devoted to genetic research at the Liggins Institute and the Malaghan Institute. During the last decade, they have made exciting discoveries demonstrating the diversified feedback loops and communication within the body’s genetic network. They could have alerted the government to the possible effects of mRNA vaccines on immune responses and organ systems. Indeed, there were many other geneticists overseas issuing such warnings. The simple point is that well known cautionary gene therapy research findings should have alerted our government advisors to the possibility of severe adverse reactions to genetically active vaccines.
Finally, there have been problems generated through the overreach of government authority. Power is not a problem in itself, but if the government has the power to favour those supporting its views and punish those dissenting, then there is an imbalance in power that can be exploited. If media independence and information can be controlled and the protections of the Bill of Rights also are ignored, if autonomous regulators are required to agree with government information, if the courts feel obliged to accept the assurances of safety provided by the government alone, political disinformation can become institutionalised into the fabric of daily administration of society.
A time for national reconciliation
I am writing this release before Christmas because many kiwi families are doing it hard. Some have lost their breadwinner or mother, a few have lost a child. Others are struggling with debilitating adverse effects and an uncertain future. All were good people who trusted government messaging about safety. Thousands of people have become ill with new health conditions. Their predicament is unsung because, apparently, the government craves a clean sheet for public consumption. Others were forced or ‘persuaded’ into it by mandates. Seven people have died this year from Covid, while the graphical data points to hundreds of individuals who have died in the 60+ cohort in the week following vaccination. Certainly more than our most significant historical disasters outside of wartime. Tens of thousands more have experienced adverse effects. Their long term prognosis is unknown.
Now is the time to acknowledge their sacrifice and make amends. This will involve asking a lot of searching questions within the MoH and the government. It will require a reexamination of cases and data. Certainty was forcefully expressed to the public when science dictated caution. It could involve a Royal Commission of Inquiry, but this lengthy process will not address immediate concerns. Indeed, the NZ Bill of Rights should be ‘entrenched’ as a constitutional provision beyond the reach of parliament alone to alter. This will strengthen the individual rights that the judiciary can protect. A change of heart among a strangely compliant mainstream media is also required. An honest statement of apology and a commitment to immediately address the severe shortcomings discussed here is called for. Disinformation has unnecessarily divided our nation.
Guy Hatchard, PhD, is a former senior manager at Genetic ID. His research work has looked at the influence of human factors on social and economic indicators. Find him on Facebook here.

{kind=link}